Home Remedies For Foot Bunions
Overview
 The classic bunion is a bump on the side of the great toe joint. This bump represents an actual deviation of the 1st metatarsal. In addition, there is also deviation of the great toe toward the second toe. In severe cases, the great toe can either lie above or below the second toe.
The classic bunion is a bump on the side of the great toe joint. This bump represents an actual deviation of the 1st metatarsal. In addition, there is also deviation of the great toe toward the second toe. In severe cases, the great toe can either lie above or below the second toe.
Causes
Foot problems typically develop in early adulthood and get worse as the foot spreads with aging. For many people, bunions run in the family. They may be just one of several problems due to weak or poor foot structure. Bunions sometimes develop with arthritis. In people with leg length discrepancies, bunions usually form in the longer leg. Women are especially prone to developing bunions. Years of wearing tight, poorly fitting shoes especially high-heeled, pointed shoes can bring on bunions. Such shoes gradually push the foot bones into an unnatural shape.
Symptoms
The symptoms of hallux valgus usually center on the bunion. The bunion is painful. The severe hallux valgus deformity is also distressing to many and becomes a cosmetic problem. Finding appropriate shoe wear can become difficult, especially for women who want to be fashionable but have difficulty tolerating fashionable shoe wear. Finally, increasing deformity begins to displace the second toe upward and may create a situation where the second toe is constantly rubbing on the shoe.
Diagnosis
Bunions are readily apparent, you can see the prominence at the base of the big toe or side of the foot. However, to fully evaluate your condition, the Podiatrist may arrange for x-rays to be taken to determine the degree of the deformity and assess the changes that have occurred. Because bunions are progressive, they don't go away, and will usually get worse over time. But not all cases are alike, some bunions progress more rapidly than others. There is no clear-cut way to predict how fast a bunion will get worse. The severity of the bunion and the symptoms you have will help determine what treatment is recommended for you.
Non Surgical Treatment
Some bunions can be treated without surgery. If you have a bunion, wear shoes that are roomy enough so that they won?t put pressure on it. You can choose to have your shoes stretched out professionally or try cushioning the painful area with protective pads. Orthotics have been shown to help prevent progression of bunions. Oral nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, may be recommended to reduce pain and inflammation. Applying an ice pack several times a day can also help reduce inflammation and pain. If your bunion progresses to a point where you have difficulty walking or experience pain even with accommodative shoes, surgery may be necessary. 
Surgical Treatment
Surgery is the only way to correct a bunion. A bunion will usually get worse over time, so if it's left untreated it's likely to get bigger and become more painful. If your bunion is causing a significant amount of pain and affecting your quality of life, your GP may refer you to be assessed for bunion surgery. The aim of surgery is to relieve pain and improve the alignment of your big toe. Surgery isn't usually carried out for cosmetic reasons alone. Even after surgery, there may still be limits to the styles of shoe you can wear. Bunion surgery is often carried out as a day procedure, which means you won't have to stay in hospital overnight. The procedure will either be carried out under a local anaesthetic or a general anaesthetic.
What Is Overpronation Of The Foot
Overview
Pronation is a normal motion that our feet make as they walk. With each step, the heel touches the ground first, then the foot rolls forward to the toes, causing the ankle to roll inward slightly and the arch to flatten out. That?s normal. But when that rolling inward becomes more pronounced, that?s over-pronation, which is a big problem. You can usually see over-pronation by looking at the back of the leg and foot. The Achilles tendon normally runs straight down from the leg to the foot, hitting the floor at a perpendicular angle. In feet that over-pronate, the Achilles tendon will be at a slight angle to the ground and the ankle bone will appear more prominent than usual.
Causes
Abnormal foot biomechanics usually causes over-use type injuries, occurring most frequently in runners. When a neutral foot pronates during walking or running, the lower leg, knee and thigh all rotate internally (medially). When an athlete with an overpronated foot runs, this rotation movement is exaggerated and becomes more marked.
Symptoms
Eventually, over-pronation can lead to a full list of maladies including flat feet, plantar fasciitis, plantar fibroma, neuromas, heel spurs, shin splints, ankle sprains, bunions, hammertoes, calluses, and pain in the arches, knee, hip and lower back. But it doesn?t have to go that far, because there are steps we can take to correct the over-pronation. In the vast majority of cases, we?ll prescribe custom foot orthotics, which will realign your ankles, redistribute the weight, support the arch and reduce the twisting. Many orthotics will fit snugly into your normal shoes. Although we?ll also take a look at the type of shoes you wear to see if they are contributing to the problem.
Diagnosis
So, how can you tell if you have overpronation, or abnormal motion in your feet, and what plantar fasciitis treatment will work to correct it? Look at your feet. While standing, do you clearly see the arch on the inside of your foot? If not, and if the innermost part of your sole touches the floor, then your feet are overpronated. Look at your (running/walking) shoes. If your shoes are more worn on the inside of the sole in particular, then pronation may be a problem for you. Use the wet foot test. Wet your feet and walk along a section of pavement, then look at the footprints you leave behind. A normal foot will leave a print of the heel connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot.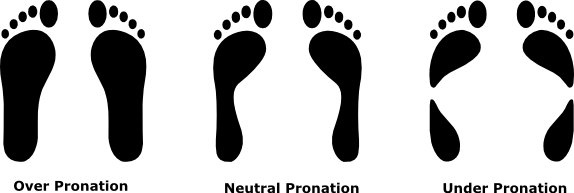
Non Surgical Treatment
If a young child is diagnosed with overpronation braces and custom orthotics can be, conjunction with strengthening and stretching exercises, to realign the bones of the foot. These treatments may have to continue until the child has stopped growing, and orthotics may need to be worn for life in order to prevent the foot reverting to an overpronated state. Wearing shoes that properly support the foot, particularly the arch, is one of the most effective treatments for overpronation. Custom-made orthotic inserts can also be very beneficial. They too support the arch and distribute body weight correctly throughout the foot. Motion-control shoes that prohibit pronation can be worn, so may be useful for those with severe overpronation. One good treatment is to walk barefoot as often as possible. Not relying on shoes to support the arch will encourage proper muscle use. Practicing yoga can help to correct poor posture and teach you how to stand with your weight balanced evenly across the whole foot.
Surgical Treatment
Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults.
An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer.
Pronation is a normal motion that our feet make as they walk. With each step, the heel touches the ground first, then the foot rolls forward to the toes, causing the ankle to roll inward slightly and the arch to flatten out. That?s normal. But when that rolling inward becomes more pronounced, that?s over-pronation, which is a big problem. You can usually see over-pronation by looking at the back of the leg and foot. The Achilles tendon normally runs straight down from the leg to the foot, hitting the floor at a perpendicular angle. In feet that over-pronate, the Achilles tendon will be at a slight angle to the ground and the ankle bone will appear more prominent than usual.
Causes
Abnormal foot biomechanics usually causes over-use type injuries, occurring most frequently in runners. When a neutral foot pronates during walking or running, the lower leg, knee and thigh all rotate internally (medially). When an athlete with an overpronated foot runs, this rotation movement is exaggerated and becomes more marked.
Symptoms
Eventually, over-pronation can lead to a full list of maladies including flat feet, plantar fasciitis, plantar fibroma, neuromas, heel spurs, shin splints, ankle sprains, bunions, hammertoes, calluses, and pain in the arches, knee, hip and lower back. But it doesn?t have to go that far, because there are steps we can take to correct the over-pronation. In the vast majority of cases, we?ll prescribe custom foot orthotics, which will realign your ankles, redistribute the weight, support the arch and reduce the twisting. Many orthotics will fit snugly into your normal shoes. Although we?ll also take a look at the type of shoes you wear to see if they are contributing to the problem.
Diagnosis
So, how can you tell if you have overpronation, or abnormal motion in your feet, and what plantar fasciitis treatment will work to correct it? Look at your feet. While standing, do you clearly see the arch on the inside of your foot? If not, and if the innermost part of your sole touches the floor, then your feet are overpronated. Look at your (running/walking) shoes. If your shoes are more worn on the inside of the sole in particular, then pronation may be a problem for you. Use the wet foot test. Wet your feet and walk along a section of pavement, then look at the footprints you leave behind. A normal foot will leave a print of the heel connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot.
Non Surgical Treatment
If a young child is diagnosed with overpronation braces and custom orthotics can be, conjunction with strengthening and stretching exercises, to realign the bones of the foot. These treatments may have to continue until the child has stopped growing, and orthotics may need to be worn for life in order to prevent the foot reverting to an overpronated state. Wearing shoes that properly support the foot, particularly the arch, is one of the most effective treatments for overpronation. Custom-made orthotic inserts can also be very beneficial. They too support the arch and distribute body weight correctly throughout the foot. Motion-control shoes that prohibit pronation can be worn, so may be useful for those with severe overpronation. One good treatment is to walk barefoot as often as possible. Not relying on shoes to support the arch will encourage proper muscle use. Practicing yoga can help to correct poor posture and teach you how to stand with your weight balanced evenly across the whole foot.
Surgical Treatment
Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults.
An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer.
Tips On How To Diagnose Severs Disease?
Overview
What Is Calcaneal Apophysitis? Calcaneal apophysitis is a painful inflammation of the heel?s growth plate. It typically affects children between the ages of 8 and 14 years old, because the heel bone (calcaneus) is not fully developed until at least age 14. Until then, new bone is forming at the growth plate (physis), a weak area located at the back of the heel. When there is too much repetitive stress on the growth plate, inflammation can develop. Calcaneal apophysitis is also called Sever?s disease, although it is not a true ?disease.? It is the most common cause of heel pain in children, and can occur in one or both feet. Heel pain in children differs from the most common type of heel pain experienced by adults. While heel pain in adults usually subsides after a period of walking, pediatric heel pain generally doesn?t improve in this manner. In fact, walking typically makes the pain worse.
Causes
There are many biomechanical factors that predispose a young athlete to calcaneal apophysitis. The majority of patients will present with an ankle equinus deformity, which ultimately exerts an increased pulling force to the Achilles insertion and non-ossified apophysis. Furthermore, patients may present with hyperpronation of the rearfoot. This allows more of a ?teeter-totter? effect or lack of motion control on the frontal plane of the calcaneus.
Symptoms
The pain associated with Sever's disease is usually felt along the back of the heel and becomes worse when running or walking. In some children, the pain is so severe they may limp when walking. One of the diagnostic tests for Sever's disease is the "squeeze test". Squeezing both sides of the heel together will produce immediate discomfort. Many children feel pain immediately upon waking and may have calf muscle stiffness in the morning.
Diagnosis
Sever condition is diagnosed by detecting the characteristic symptoms and signs above in the older children, particularly boys between 8 and 15 years of age. Sometimes X-ray testing can be helpful as it can occasionally demonstrate irregularity of the calcaneus bone at the point where the Achilles tendon attaches.
Non Surgical Treatment
The physiotherapist will thoroughly assess the affected areas and general mechanics to determine what factors may be contributing, also to rule out any other injuries or stress fractures, etc. Treatment focusing on the affected area will consist of modified rest, ice, massage, stretches and electrotherapy. A foam heel raise may also be given to help decrease pain. The physiotherapist may also treat other areas if biomechanical problems are noted. This may include massage, mobilization and exercises to stretch and strengthen certain areas. They may also refer the patient to see a podiatrist if they believe the foot posture is a factor.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
What Is Calcaneal Apophysitis? Calcaneal apophysitis is a painful inflammation of the heel?s growth plate. It typically affects children between the ages of 8 and 14 years old, because the heel bone (calcaneus) is not fully developed until at least age 14. Until then, new bone is forming at the growth plate (physis), a weak area located at the back of the heel. When there is too much repetitive stress on the growth plate, inflammation can develop. Calcaneal apophysitis is also called Sever?s disease, although it is not a true ?disease.? It is the most common cause of heel pain in children, and can occur in one or both feet. Heel pain in children differs from the most common type of heel pain experienced by adults. While heel pain in adults usually subsides after a period of walking, pediatric heel pain generally doesn?t improve in this manner. In fact, walking typically makes the pain worse.
Causes
There are many biomechanical factors that predispose a young athlete to calcaneal apophysitis. The majority of patients will present with an ankle equinus deformity, which ultimately exerts an increased pulling force to the Achilles insertion and non-ossified apophysis. Furthermore, patients may present with hyperpronation of the rearfoot. This allows more of a ?teeter-totter? effect or lack of motion control on the frontal plane of the calcaneus.
Symptoms
The pain associated with Sever's disease is usually felt along the back of the heel and becomes worse when running or walking. In some children, the pain is so severe they may limp when walking. One of the diagnostic tests for Sever's disease is the "squeeze test". Squeezing both sides of the heel together will produce immediate discomfort. Many children feel pain immediately upon waking and may have calf muscle stiffness in the morning.
Diagnosis
Sever condition is diagnosed by detecting the characteristic symptoms and signs above in the older children, particularly boys between 8 and 15 years of age. Sometimes X-ray testing can be helpful as it can occasionally demonstrate irregularity of the calcaneus bone at the point where the Achilles tendon attaches.
Non Surgical Treatment
The physiotherapist will thoroughly assess the affected areas and general mechanics to determine what factors may be contributing, also to rule out any other injuries or stress fractures, etc. Treatment focusing on the affected area will consist of modified rest, ice, massage, stretches and electrotherapy. A foam heel raise may also be given to help decrease pain. The physiotherapist may also treat other areas if biomechanical problems are noted. This may include massage, mobilization and exercises to stretch and strengthen certain areas. They may also refer the patient to see a podiatrist if they believe the foot posture is a factor.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Have I Suffered A Ruptured Achilles Tendon?
Overview
 The largest tendon in the body, the Achilles tendon is a cord connecting the calf muscles to the heel bone. Also called the ?cord of Achilles,? the tendon gets its name from the hero of Greek myth. According to legend, Achilles was invulnerable everywhere but his heel, where a poisoned arrow eventually felled him. Because the blood supply to the Achilles tendon lessens with age, the tendon becomes vulnerable to inflammation and rupture, a fact which makes it a true ?Achilles heel? for many older patients. Achilles tendon injuries are also common among athletes and those who engage in more physically demanding activity.
The largest tendon in the body, the Achilles tendon is a cord connecting the calf muscles to the heel bone. Also called the ?cord of Achilles,? the tendon gets its name from the hero of Greek myth. According to legend, Achilles was invulnerable everywhere but his heel, where a poisoned arrow eventually felled him. Because the blood supply to the Achilles tendon lessens with age, the tendon becomes vulnerable to inflammation and rupture, a fact which makes it a true ?Achilles heel? for many older patients. Achilles tendon injuries are also common among athletes and those who engage in more physically demanding activity.
Causes
Factors that may increase your risk of Achilles tendon rupture include Age. The peak age for Achilles tendon rupture is 30 to 40. Your sex. Achilles tendon rupture is up to five times more likely to occur in men than in women. Playing recreational sports. Achilles tendon injuries occur more often in sports that involve running, jumping and sudden starts and stops - such as soccer, basketball and tennis. Steroid injections. Doctors sometimes inject steroids into an ankle joint to reduce pain and inflammation. However, this medication can weaken nearby tendons and has been associated with Achilles tendon ruptures. Certain antibiotics. Fluoroquinolone antibiotics, such as ciprofloxacin (Cipro) or levofloxacin (Levaquin), increase the risk of Achilles tendon rupture.
Symptoms
An Achilles tendon rupture is when the tendon that connects the heel bone to the calf muscle tears and the fibers separate. This happens mostly between the ages of 30 and 50, and usually is caused by sports. Symptoms of Achilles tendon rupture include the following. A pop or snap when the tendon tears. Severe pain in back of the ankle, making it nearly impossible to walk. Swelling and discoloration. Tenderness. Inability to rise on toes. A gap in the back of the ankle where the tendons are separated.
Diagnosis
A consultation and physical exam with a qualified musculoskeletal expert is the first step. X-ray or MRI scanning may be required for a diagnosis. Once a rupture is diagnosed it should be treated to prevent loss of strength and inadequate healing.
Non Surgical Treatment
The best treatment for a ruptured Achilles tendon often depends on your age, activity level and the severity of your injury. In general, younger and more active people often choose surgery to repair a completely ruptured Achilles tendon while older people are more likely to opt for nonsurgical treatment. Recent studies, however, have shown fairly equal effectiveness of both operative and nonoperative management. Nonsurgical treatment. This approach typically involves wearing a cast or walking boot with wedges to elevate your heel; this allows the ends of your torn tendon to heal. This method can be effective, and it avoids the risks, such as infection, associated with surgery. However, the likelihood of re-rupture may be higher with a nonsurgical approach, and recovery can take longer. If re-rupture occurs, surgical repair may be more difficult. 
Surgical Treatment
The goal of surgery is to realign the two ends of the ruptured tendon to allow healing. There are multiple techniques to accomplish this goal that will vary from surgeon to surgeon. Recovery from this injury is usually very successful with return to full function in approximately 6 months. Post operatively casting is required with the use of crutches or other means to remain non-weightbearing for 4-8 weeks. This is followed by a course of physical therapy. Partial rupture may or may not require surgical intervention depending on the extent of injury but cast immobilization is a common requirement.
Prevention
To help reduce your chance of getting Achilles tendon rupture, take the following steps. Do warm-up exercises before an activity and cool down exercises after an activity. Wear proper footwear. Maintain a healthy weight. Rest if you feel pain during an activity. Change your routine. Switch between high-impact activities and low-impact activities. Strengthen your calf muscle with exercises.
True Vs. Functional Leg Length Discrepancy
Overview
Leg length discrepancies are differences between the lengths of your legs. Not only can the actual difference vary from person to person but also how much it affects daily life. Small discrepancies often go unnoticed and do not need to be treated. Larger differences may affect posture or cause a limp during walking. The discrepancy may be from the upper leg bone (femur) or the lower leg bone (tibia).
Causes
Leg length discrepancies can be caused by poor alignment of the pelvis or simply because one leg is structurally longer than the other. Regardless of the reason, your body wants to be symmetrical and will do its best to compensate for the length difference. The greater the leg length difference, the earlier the symptoms will present themselves to the patient. Specific diagnoses that coincide with leg length discrepancy include: scoliosis, lumbar herniated discs, sacroiliitis, pelvic obiliquity, greater trochanteric bursitis, hip arthritis, piriformis syndrome, patellofemoral syndrome and foot pronation. Other potential causes could be due to an injury (such as a fracture), bone disease, bone tumors, congenital problems (present at birth) or from a neuromuscular problem.
Symptoms
Patients with significant lower limb length discrepancies may walk with a limp, have the appearance of a curved spine (non-structural scoliosis), and experience back pain or fatigue. In addition, clothes may not fit right.
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
For minor limb length discrepancy in patients with no deformity, treatment may not be necessary. Because the risks may outweigh the benefits, surgical treatment to equalize leg lengths is usually not recommended if the difference is less than 1 inch. For these small differences, the physician may recommend a shoe lift. A lift fitted to the shoe can often improve walking and running, as well as relieve any back pain that may be caused by the limb length discrepancy. Shoe lifts are inexpensive and can be removed if they are not effective.

Surgical Treatment
Your child will be given general anesthetic. We cut the bone and insert metal pins above and below the cut. A metal frame is attached to the pins to support the leg. Over weeks and months, the metal device is adjusted to gradually pull the bone apart to create space between the ends of the bones. New bone forms to fill in the space, extending the length of the bone. Once the lengthening process is completed and the bones have healed, your child will require one more short operation to remove the lengthening device. We will see your child regularly to monitor the leg and adjust the metal lengthening device. We may also refer your child to a physical therapist to ensure that he or she stays mobile and has full range of motion in the leg. Typically, it takes a month of healing for every centimeter that the leg is lengthened.
Leg length discrepancies are differences between the lengths of your legs. Not only can the actual difference vary from person to person but also how much it affects daily life. Small discrepancies often go unnoticed and do not need to be treated. Larger differences may affect posture or cause a limp during walking. The discrepancy may be from the upper leg bone (femur) or the lower leg bone (tibia).
Causes
Leg length discrepancies can be caused by poor alignment of the pelvis or simply because one leg is structurally longer than the other. Regardless of the reason, your body wants to be symmetrical and will do its best to compensate for the length difference. The greater the leg length difference, the earlier the symptoms will present themselves to the patient. Specific diagnoses that coincide with leg length discrepancy include: scoliosis, lumbar herniated discs, sacroiliitis, pelvic obiliquity, greater trochanteric bursitis, hip arthritis, piriformis syndrome, patellofemoral syndrome and foot pronation. Other potential causes could be due to an injury (such as a fracture), bone disease, bone tumors, congenital problems (present at birth) or from a neuromuscular problem.
Symptoms
Patients with significant lower limb length discrepancies may walk with a limp, have the appearance of a curved spine (non-structural scoliosis), and experience back pain or fatigue. In addition, clothes may not fit right.
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
For minor limb length discrepancy in patients with no deformity, treatment may not be necessary. Because the risks may outweigh the benefits, surgical treatment to equalize leg lengths is usually not recommended if the difference is less than 1 inch. For these small differences, the physician may recommend a shoe lift. A lift fitted to the shoe can often improve walking and running, as well as relieve any back pain that may be caused by the limb length discrepancy. Shoe lifts are inexpensive and can be removed if they are not effective.
Surgical Treatment
Your child will be given general anesthetic. We cut the bone and insert metal pins above and below the cut. A metal frame is attached to the pins to support the leg. Over weeks and months, the metal device is adjusted to gradually pull the bone apart to create space between the ends of the bones. New bone forms to fill in the space, extending the length of the bone. Once the lengthening process is completed and the bones have healed, your child will require one more short operation to remove the lengthening device. We will see your child regularly to monitor the leg and adjust the metal lengthening device. We may also refer your child to a physical therapist to ensure that he or she stays mobile and has full range of motion in the leg. Typically, it takes a month of healing for every centimeter that the leg is lengthened.
Symptoms Of Flat Feet In Adults
Overview The posterior tibialis muscle originates on the bones of the leg (tibia and fibula). This muscle then passes behind the medial (inside) aspect of the ankle and attaches to the medial midfoot as the posterior tibial tendon. The posterior tibial tendon serves to invert (roll inward) the foot and maintain the arch of the foot. This tendon plays a central role in maintaining the normal alignment of the foot and also in enabling normal gait (walking). In addition to tendons running across the ankle and foot joints, a number of ligaments span and stabilize these joints. The ligaments at the medial ankle can become stretched and contribute to the progressive flattening of the arch. Several muscles and tendons around the ankle and foot act to counter-balance the action of the posterior tibial tendon. Under normal circumstances, the result is a balanced ankle and foot with normal motion. When the posterior tibial tendon fails, the other muscles and tendons become relatively over-powering. These muscles then contribute to the progressive deformity seen with this disorder.  Causes As discussed above, many health conditions can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to hold up the arch and support your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch. Symptoms Many patients with this condition have no pain or symptoms. When problems do arise, the good news is that acquired flatfoot treatment is often very effective. Initially, it will be important to rest and avoid activities that worsen the pain. Diagnosis Perform a structural assessment of the foot and ankle. Check the ankle for alignment and position. When it comes to patients with severe PTTD, the deltoid has failed, causing an instability of the ankle and possible valgus of the ankle. This is a rare and difficult problem to address. However, if one misses it, it can lead to dire consequences and potential surgical failure. Check the heel alignment and position of the heel both loaded and during varus/valgus stress. Compare range of motion of the heel to the normal contralateral limb. Check alignment of the midtarsal joint for collapse and lateral deviation. Noting the level of lateral deviation in comparison to the contralateral limb is critical for surgical planning. Check midfoot alignment of the naviculocuneiform joints and metatarsocuneiform joints both for sag and hypermobility. Non surgical Treatment Flatfoot deformity can be treated conservatively or with surgical intervention depending on the severity of the condition. When people notice their arches flattening, they should immediately avoid non-supportive shoes such as flip-flops, sandals or thin-soled tennis shoes. Theses shoes will only worsen the flatfoot deformity and exacerbate arch pain. Next, custom orthotics are essential for people with collapsed arches. Over-the-counter insoles only provide cushion and padding to the arch, whereas custom orthotics are fabricated to specifically fit the patient?s foot and provide support in the arch where the posterior tibial tendon is unable to anymore. Use of custom orthotics in the early phases of flatfoot or PTTD can prevent worsening of symptoms and prevent further attenuation or injury to the posterior tibial tendon. In more severe cases of flatfoot deformity an ankle foot orthosis (AFO) such as a Ritchie brace is needed. This brace provides more support to the arch and hindfoot rather than an orthotic but can be bulky in normal shoegear. Additional treatment along with use of custom orthotics is use of non-steroidal anti-inflammatories (NSAIDS) such as Advil, Motrin, or Ibuprofen which can decrease inflammation to the posterior tibial tendon. If pain is severe, the patient may need to be placed in a below the knee air walker boot for several weeks which will allow the tendon to rest and heal, especially if a posterior tibial tendon tear is noted on MRI.
Causes As discussed above, many health conditions can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to hold up the arch and support your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch. Symptoms Many patients with this condition have no pain or symptoms. When problems do arise, the good news is that acquired flatfoot treatment is often very effective. Initially, it will be important to rest and avoid activities that worsen the pain. Diagnosis Perform a structural assessment of the foot and ankle. Check the ankle for alignment and position. When it comes to patients with severe PTTD, the deltoid has failed, causing an instability of the ankle and possible valgus of the ankle. This is a rare and difficult problem to address. However, if one misses it, it can lead to dire consequences and potential surgical failure. Check the heel alignment and position of the heel both loaded and during varus/valgus stress. Compare range of motion of the heel to the normal contralateral limb. Check alignment of the midtarsal joint for collapse and lateral deviation. Noting the level of lateral deviation in comparison to the contralateral limb is critical for surgical planning. Check midfoot alignment of the naviculocuneiform joints and metatarsocuneiform joints both for sag and hypermobility. Non surgical Treatment Flatfoot deformity can be treated conservatively or with surgical intervention depending on the severity of the condition. When people notice their arches flattening, they should immediately avoid non-supportive shoes such as flip-flops, sandals or thin-soled tennis shoes. Theses shoes will only worsen the flatfoot deformity and exacerbate arch pain. Next, custom orthotics are essential for people with collapsed arches. Over-the-counter insoles only provide cushion and padding to the arch, whereas custom orthotics are fabricated to specifically fit the patient?s foot and provide support in the arch where the posterior tibial tendon is unable to anymore. Use of custom orthotics in the early phases of flatfoot or PTTD can prevent worsening of symptoms and prevent further attenuation or injury to the posterior tibial tendon. In more severe cases of flatfoot deformity an ankle foot orthosis (AFO) such as a Ritchie brace is needed. This brace provides more support to the arch and hindfoot rather than an orthotic but can be bulky in normal shoegear. Additional treatment along with use of custom orthotics is use of non-steroidal anti-inflammatories (NSAIDS) such as Advil, Motrin, or Ibuprofen which can decrease inflammation to the posterior tibial tendon. If pain is severe, the patient may need to be placed in a below the knee air walker boot for several weeks which will allow the tendon to rest and heal, especially if a posterior tibial tendon tear is noted on MRI.  Surgical Treatment If surgery is necessary, a number of different procedures may be considered. The specifics of the planned surgery depend upon the stage of the disorder and the patient?s specific goals. Procedures may include ligament and muscle lengthening, removal of the inflamed tendon lining, tendon transfers, cutting and realigning bones, placement of implants to realign the foot and joint fusions. In general, early stage disease may be treated with tendon and ligament (soft-tissue) procedures with the addition of osteotomies to realign the foot. Later stage disease with either a rigidly fixed deformity or with arthritis is often treated with fusion procedures. If you are considering surgery, your doctor will speak with about the specifics of the planned procedure.
Surgical Treatment If surgery is necessary, a number of different procedures may be considered. The specifics of the planned surgery depend upon the stage of the disorder and the patient?s specific goals. Procedures may include ligament and muscle lengthening, removal of the inflamed tendon lining, tendon transfers, cutting and realigning bones, placement of implants to realign the foot and joint fusions. In general, early stage disease may be treated with tendon and ligament (soft-tissue) procedures with the addition of osteotomies to realign the foot. Later stage disease with either a rigidly fixed deformity or with arthritis is often treated with fusion procedures. If you are considering surgery, your doctor will speak with about the specifics of the planned procedure.